
Standers support those unable to maintain an aligned weight-bearing posture safely. For children with cerebral palsy (CP) classified at Gross Motor Function Classification System (GMFCS) levels IV or V, standers provide an important change of position with psycho-social benefits, increasing visual access, communication and interaction with others. The strongest research evidence currently suggests that supported standing can maintain or enhance bone-mineral density (BMD), and help to prevent development of contractures. Lower quality evidence suggests positive impacts on other outcomes such as bowel function, hip stability and functional abilities.1
In children with CP, muscle starts to differ from typically developing children before 12 months, with lifetime implications for muscle physiology, metabolic health and function.2 This reinforces that standing must be introduced when children typically begin pulling to stand and standing with their caregivers (9-12 months) to promote muscle and bone development. Supported-standing increases metabolic demand and heart rate (exercise) for children at GMFCS IV-V, and 60-minutes daily use is recommended to reduce sedentary behavior (click here for PDF). Supported-standing can increase child participation, and achievement of child and family goals if integrated into age-appropriate and meaningful activities and routines. Standers should be carefully selected to suit the physical and the social environment (see figure 1) as well as to meet the postural needs of the child.3

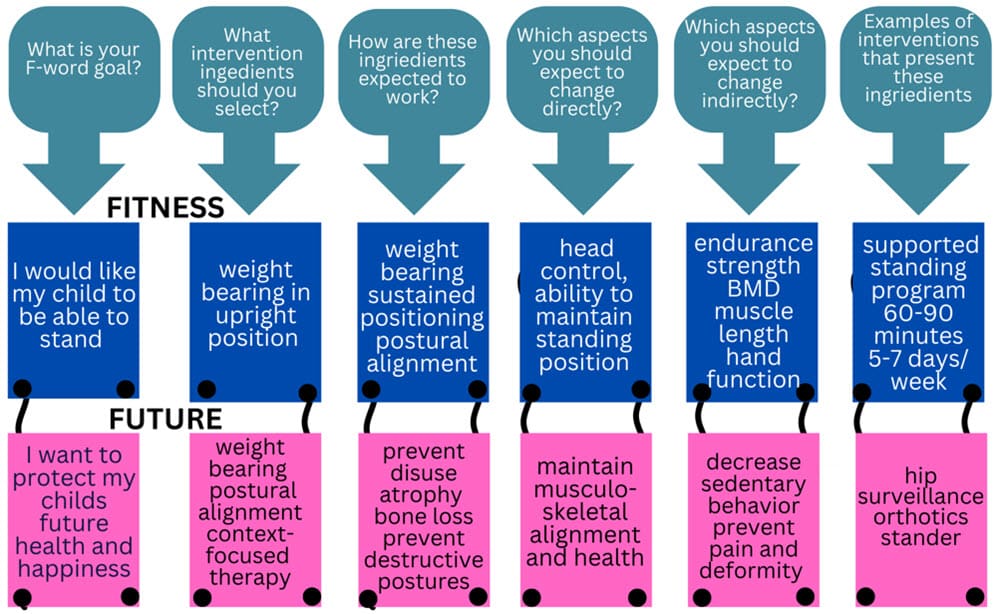
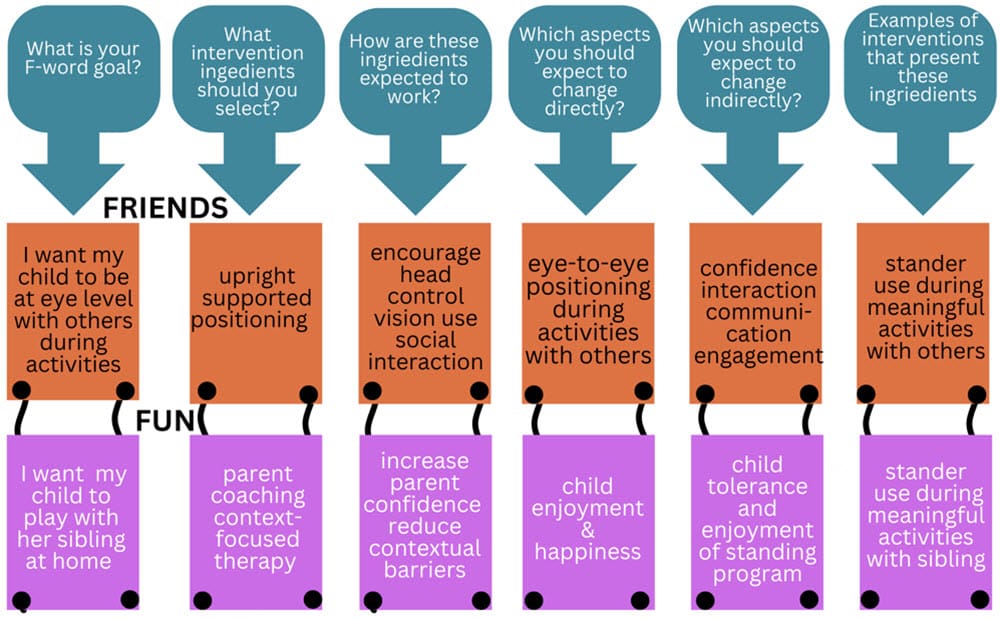
This case report describes the successful implementation of a supported-standing intervention to address multiple therapeutic goals. The F-words (functioning, family, fitness, fun, friends, future) help us focus on child and family strengths and promoting childhood development.4 Hercules Leite and his team in Brazil developed the F-words Lens Tool to help the therapists, caregivers and users examine the mechanisms of action for different therapeutic interventions.5 In this article we use this tool to examine stander use with a young child.
Case Presentation:
When we first met Pheobe, she was a 9-month-old girl diagnosed with tetraplegic cerebral palsy (CP). She was born full term after an uncomplicated pregnancy and diagnosed with hypoxic ischemic encephalopathy. While most infants with this diagnosis receive cooling therapy, Pheobe was not offered this intervention. She exhibited low tone trunk (hypotonia), spastic extremities and dystonia. Her Hammersmith Infant Neurological Exam (HINE) score at 9 months was 15, with an asymmetry score of 11, and a hypotonia score of 0.32. These scores indicated that she would most likely have motor skills at the GMFCS IV/V range, need targeted hand therapy such as constraint induced movement therapy (CIMT) and bimanual therapy, and benefit from hypotonia-specific interventions (see AACPDM hypotonia care pathway and the Hypotonia Wheel.
Intervention:
A Prime Engineering Superstand HLT Early Intervention Model was chosen because it accommodates very small children, provides a lot of growth, and has many options for postural support. This was set up in a supine position, with head, trunk, hip, knee and foot supports. A tray was used for upper limb support and to promote functioning.
The primary goals of this intervention are mapped out using the F-word Lens tool.
Fitness and Future (prevent known harms):
A recent overview of postural interventions concluded that high-quality evidence supports use of standers to improve BMD in children with CP.6 Children at GMFCS IV and V are at highest risk for contracture and windswept hip deformity and the HLT Superstand can be adjusted to accommodate contractures (with a contracture bracket) and even improve range of motion,7 should this be necessary in future. A large Swedish cohort study has determined that the most at-risk joint is the knee, followed by the hip for children at GMFCS V.8 Preventing hip and knee flexion contractures is important because these are associated with windswept hip deformity.9
Children classified at GMFCS IV or V are at the highest risk of hip subluxation and dislocation. Standing with the hips in 20-30 degrees abduction is recommended,10 although some low-quality studies (at high risk-of-bias) have suggested as much as 60 degrees.11–14 The private and school-based early intervention providers agreed to position Phoebe in 10-15 degrees hip abduction on each leg (20-30 total), since this appeared to be well-tolerated. Excessive abduction can lead to pain and may decrease weight bearing.15 While daily standing may help slow the progression of hip subluxation,16 90% of children at GMFCS V and 70% at GMFCS IV are anticipated to require surgical intervention. 17 Surgery should not be considered a failure, but rather a preventive intervention, and has been shown in large population studies to reduce pain and deformity, and increase function.18
Functioning, Family, Fun and Friends:
A variety of activities were used to facilitate Phoebe’s upper extremity development, including reach, grasp, and manipulation of objects for play and activities of daily living. A sock was used as a soft restraint on Phoebe’s right hand to encourage use of her less able left hand (click here). At other times, activities that required two hands were targeted (see CPtoys.com for ideas). The stander was incorporated into preferred activities and routines to assist in meeting family goals for participation (see figures 2-4 below).

Implementation:
The stander was introduced gradually, starting with short sessions and gradually increasing duration and frequency. Phoebe’s response was closely monitored, and adjustments made to the positioning and supports to make sure she was comfortable and well-aligned. Favorite activities such as pretend play with her doll were used to make standing a fun and enjoyable time. The height of the stander allowed Phoebe to stand at kitchen counter height while her Mom prepared meals, and she enjoyed some finger food snacks.

Outcomes:
Phoebe demonstrated increased weight-bearing through the lower extremities during standing sessions at the couch, and sit-to-stand practice. Hip surveillance x-rays at 18 months revealed 35 and 40% migration percentages. However, her orthopedic surgeon noted no further progression by age 3 years with no hip or knee contractures or pain.
Phoebe demonstrated enhanced upper extremity function, with increased reach, grasp, manipulation of objects, and ability to self-feed during stander use. Engagement increased during standing sessions, including interacting with her sibling and caregivers and using her augmentative communication device. The family reported positive experiences with the stander and expressed satisfaction with her progress.
At age 24 months, Phoebe’s Gross Motor Function Measure-88 raw score was 8 without devices, and 20 when using her orthotics, stander and stepping device. By scoring the GMFM-88 with and without assistive devices, we could demonstrate to the third-party payer that multiple devices were needed to enhance function.
Conclusion:
This case report demonstrates the potential benefits of incorporating standers into early intervention for children with CP. By addressing multiple therapeutic goals simultaneously, including bone health, contracture prevention, and functional participation, standers can significantly enhance developmental outcomes.

Roslyn may be reached at roslivingstone@gmail.com.
Roslyn Livingstone is an occupational therapist with more than 30 years’ clinical experience specializing in assistive technology, positioning and mobility assessment for children with multiple and complex disabilities. Her clinically based research has focused on the use and introduction of power mobility with young children. She has extensively published evidence related to the use of power mobility, seating, standing and stepping devices, particularly for children with non-ambulant cerebral palsy, and has presented nationally and internationally on these topics. Livingstone lives in rural British Columbia with her husband and dogs and is a clinical assistant professor with University of British Columbia.

Ginny may be reached at ginny@paleg.com
Ginny Paleg, PT, MPT, DScPT, is a pediatric physiotherapist based in Silver Spring, Maryland, USA. With over 20 years of experience, she specializes in working with infants and young children (0-3 years) in home and childcare settings, focusing on the F-words framework to guide her practice. Paleg earned her master’s in physical therapy from Emory University and her Doctorate in Physical Therapy from the University of Maryland Baltimore. Her clinical expertise lies in assessing and intervening for children with severe motor impairments, particularly those at GMFCS Levels IV and V. She is certified in the Prechtl General Movement Assessment (GMA) and the Hammersmith Infant Neurological Examination (HINE) and trained in Routines-Based Interventions and coaching methodologies. Paleg is a prolific researcher with over 60 peer-reviewed publications focusing on standers, supported stepping devices, and power mobility in children with complex needs.
References:
- McLean L, Paleg G, Livingstone R. Supported-standing interventions for children and young adults with non-ambulant cerebral palsy: A scoping review. Dev Med Child Neurol. 2023;65(6):754-772.
- Verschuren O, Smorenburg ARP, Luiking Y, Bell K, Barber L, Peterson MD. Determinants of muscle preservation in individuals with cerebral palsy across the lifespan: a narrative review of the literature. J Cachexia Sarcopenia Muscle. 2018;9(3):453-464. doi:10.1002/jcsm.12287
- Paleg GS, Williams SA, Livingstone RW. Supported standing and supported stepping devices for children with non-ambulant cerebral palsy: An interdependence and F-Words focus. Int J Environ Res Public Health. 2024;21:669. https://www.mdpi.com/1660-4601/21/6/669
- Rosenbaum P, Gorter JW. The “F-words” in childhood disability: I swear this is how we should think! Child Care Health Dev. 2012;38(4):457-463. doi:10.1111/j.1365-2214.2011.01338.x
- Leite HR, de Sousa Junior RR, Souto DO, et al. F-words ingredients of non-invasive interventions for young ambulant children with cerebral palsy: A scoping review. Dev Med Child Neurol. 2024;(July):1-15. doi:10.1111/dmcn.16074
- Toohey M, Blatch-Williams R, Budini K, et al. Effectiveness of postural interventions in cerebral palsy: umbrella systematic review. Paediatrics and Child Health (United Kingdom). 2024;34(8):257-278. doi:10.1016/j.paed.2024.06.003
- Capati V, Covert SY, Paleg G. Stander use for an adolescent with cerebral palsy at GMFCS level V with hip and knee contractures. Assistive Technology. 2020;32(6):335-341. doi:10.1080/10400435.2019.1579268
- Cloodt E, Lindgren A, Lauge-Pedersen H, Rodby-Bousquet E. Sequence of flexion contracture development in the lower limb: a longitudinal analysis of 1,071 children with cerebral palsy. BMC Musculoskelet Disord. 2022;23(1):1-10. doi:10.1186/s12891-022-05548-7
- Casey J, Agustsson A, Rosenblad A, Rodby-Bousquet E. Relationship between scoliosis, windswept hips and contractures with pain and asymmetries in sitting and supine in 2450 children with cerebral palsy. Disabil Rehabil. 2022;44(22):6738-6743. doi:10.1080/09638288.2021.1971308
- Paleg G, Livingstone R. Evidence-informed clinical perspectives on postural management for hip health in children and adults with non-ambulant cerebral palsy. J Pediatr Rehabil Med. 2022;15(1):39-48. doi:10.3233/prm-220002
- Martinsson C, Himmelmann K. Abducted standing in children with cerebral palsy: Effects on hip development after 7 years. Pediatric Physical Therapy. 2021;33(2):101-107. doi:10.1097/PEP.0000000000000789
- Martinsson C, Himmelmann K. Effect of weight-bearing in abduction and extension on hip stability in children with cerebral palsy. Pediatric Physical Therapy. 2011;23(2):150-157. doi:10.1097/PEP.0b013e318218efc3
- Macias-Merlo L, Bagur-Calafat C, Girabent-Farrés M, Stuberg WA. Effects of the standing program with hip abduction on hip acetabular development in children with spastic diplegia cerebral palsy. Disabil Rehabil. 2016;38(11):1075-1081. doi:10.3109/09638288.2015.1100221
- Macias-Merlo L, Bagur-Calafat C, Girabent-Farrés M, Stuberg WA. Standing programs to promote hip flexibility in children with spastic diplegic cerebral palsy. Pediatric Physical Therapy. 2015;27:243-249. doi:10.1097/PEP.0000000000000150
- Paleg G, Altizer W, Malone R, Ballard K, Kreger A. Inclination, hip abduction, orientation, and tone affect weight-bearing in standing devices. J Pediatr Rehabil Med. 2021;14(3):433-441. doi:10.3233/PRM-190660
- Rapson R, King T, Morris C, et al. Effect of different durations of using a standing frame on the rate of hip migration in children with moderate to severe cerebral palsy: a feasibility study for a randomised controlled trial. Physiotherapy. 2022;116:42-49. doi:10.1016/j.physio.2022.01.001
- Soo B, Howard JJ, Boyd RN, et al. Hip displacement in cerebral palsy. Journal of Bone and Joint Surgery. 2006;88(1):121-129. doi:10.2106/JBJS.E.00071
- Hagglund G, Alriksson-Schmidt A, Lauge-Pedersen H, Rodby-Bousquet E, Wagner P, Westbom L. Prevention of dislocation of the hip in children with cerebral palsy: 20 year results of a population-based prevention programme. Bone Joint J. 2014;96-B:1546-1552. doi:10.1302/0301-620X.87B1.15146