

To be awarded .1 CEU and a certificate upon completion of this article, click here to visit the online course, enroll, download the PDF, and take the quiz.
Introduction
While dynamic seating has been available for a long time, it remains underutilized. Seating and wheeled mobility team members have learned quite a bit over the years about its benefits and application. Clinical experience and research show that dynamic seating has far more clinical benefits than simply preventing equipment breakage. The purpose of this article is to present a dynamic seating definition and history, describe innovative changes to design and explain clinical applications of this intervention. A summary of research supporting both the need and application of dynamic seating is included and current funding challenges will be addressed. Finally, the future of this intervention will be proposed, including a paradigm shift in its application, whereby we recognize that everyone has a right to move, including those who need aggressive postural support to maintain their position.
Dynamic seating – a definition
Most wheelchairs and seating systems are static. If the client moves, they will move in relation to the seating support surfaces, which may result in a loss of their body position and posture. Dynamic seating moves with the client in response to the force they exert.
Definitions and terminology are important so that team members know exactly what assistive technology or intervention is being recommended or used. Some literature uses the term “dynamic” or “dynamic seating” to refer to other types of interventions. The International Dynamic Seating Workgroup met several times in 2018 and agreed upon a formal definition of dynamic seating. This definition was later used in the RESNA Position Paper on the Application of Dynamic Seating.
Dynamic seating is movement which occurs within the seating system and/or wheelchair frame in response to intentional or unintentional force generated by the client. Dynamic components absorb force. When client force ceases, the stored energy is returned through the dynamic component, which in turn assists the client back to a starting position (Lange, et al., 2021, p. 3).
Dynamic seating is not the same as suspension. Suspension includes components like shock absorbers and springs, located on the lower part of the frame or near the wheels, that act to dampen vibration and other forces that occur when the wheelchair is moving. Suspension is available on some manual and power wheelchairs, sometimes as an aftermarket addition. This is an important intervention with numerous clinical benefits; however, it differs from dynamic seating.
Common categories of dynamic seating include:
- Dynamic backs that open the seat-to-back angle in response to client hip extension.
- Dynamic footrests that move in response to lower extremity forces. The footrests may lengthen or telescope in a downward direction and increase the thigh to lower leg angle as the individual’s knees extend. The footplates may also move to accommodate active ankle plantar flexion or rotate outward to accommodate foot rotation.
- Dynamic head support hardware that moves in response to neck extension and rotation. This movement may be bidirectional (forward and rearward), rotational, or multidirectional.
- A combination of dynamic seating interventions can be used to allow movement at multiple joints (see Figure 1. below).

A key feature of dynamic seating is resistance. Resistance is provided by elastomers, springs, and/or hydraulics. These components provide a degree of resistance while the client moves (providing more stable, controlled movement), store energy, and then use that stored energy to return the client to their starting point. Resistance can be increased or decreased to meet an individual’s needs. Individualizing the level of resistance for each person is important so that they can activate the dynamic component, based on their strength and muscle tone, and then return to the starting position.
These dynamic components are separate from the seating system. For example, dynamic back hardware attaches between the seat rails and the back canes. It is not integrated into the seat cushion or back support. Dynamic footrests typically replace the current footrest hangers, although secondary supports (i.e., ankle straps) are typically required. Dynamic head support hardware replaces the head support mounting hardware, although head pads are still required.
Dynamic seating – a history
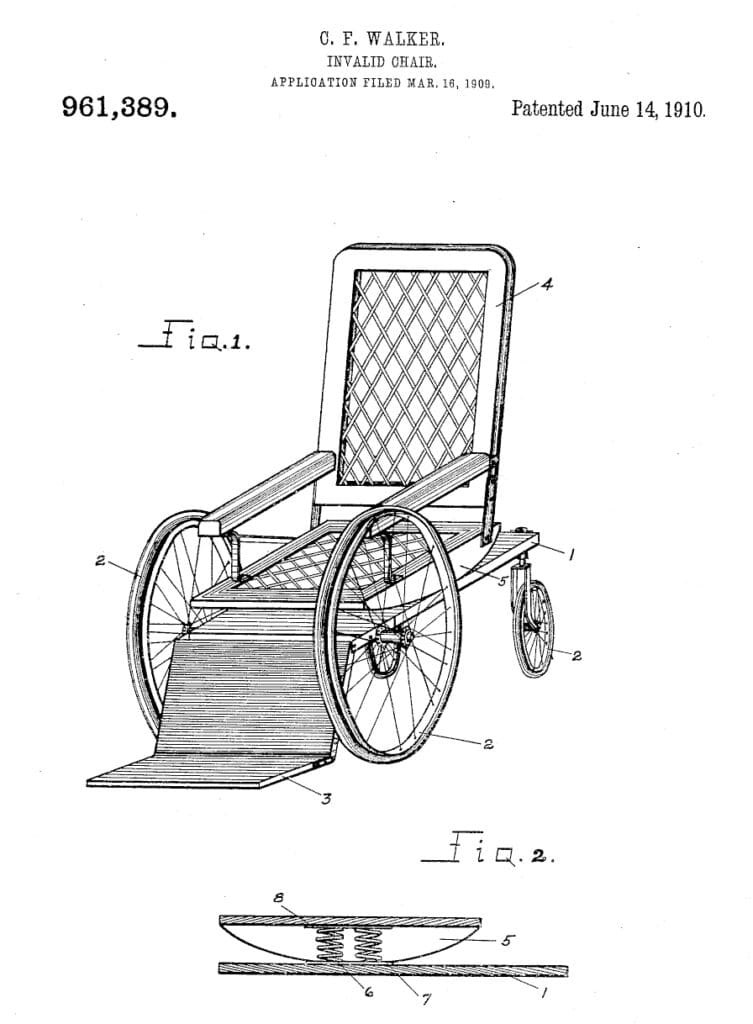
Dynamic seating options are much more readily available today compared to several years ago. Many years before commercially available options were available, some service providers fabricated homemade solutions. Various designs were proposed and patented over the years. Some early designs were intended for a stationary chair (rather than a wheelchair) but incorporated dynamic features that responded to client forces and movement. Other designs were specific to wheelchairs – either providing a rocking movement or changing the seated angles in response to client movement. In 1910, the first patent was approved for a wheelchair that moved in response to client force/movement (Charles Francis Walker, #961,389). This design used springs to provide a rocking movement (see Figure 2 below).
The first widely available wheelchair-based dynamic system, to the best of our knowledge, was the EndoFlex by Pin Dot, which was manufactured in 1989. This dynamic back provided extension of the upper portion of the back support at the lumbar area to allow the client to “lean back, stretch, or shift weight. It’s even easier to propel your wheelchair” (Pin Dot catalog, p. 37). The feature could be locked out restricting dynamic movement temporarily. The height of the entire back support could be changed to achieve the optimal height for this dynamic movement.
By 2001, several commercial options entered the market and provided a rocking movement. The Freedom Designs Spectrum wheelchair offered an option utilizing a free-floating ring to attach the back support to the back canes to allow limited back support movement in response to client force and movement. Miller’s Adaptive Technologies had two different dynamic footrest options and later added dynamic backs and dynamic head support hardware to their product line. In 2006, Degage (which eventually was renamed Seating Dynamics) began offering a dynamic back and later added dynamic footrests, as well as dynamic head support hardware. In 2008, the Kids Up Kids Rock wheelchair with integrated dynamic seating was introduced.
Dynamic seating – design
Over time, dynamic seating design has progressed in several areas. While some dynamic seating components are only compatible with the same manufacturer’s products, other components are compatible with multiple manual and power wheelchair bases, increasing access to more clients. Nearly all options in the United States are modular, rather than integrated with the wheelchair frame, allowing dynamic seating components to be retrofitted to existing wheelchairs or added to a new wheelchair. More dynamic seating components now ‘lock-out,’ preventing movement in certain situations such as during transportation. Resistance strategies have improved to provide more choices in the field and less guesswork during the ordering process.
Finally, the importance of pivot points has changed product design in recent years. It is critical that the pivot point of the dynamic component (such as a dynamic footrest), is as close as possible to the natural pivot point on the client’s body (such as the knee) (see Figure 3). This allows a ready and efficient response to client movement and force, reduces shear forces, and helps maintain client position.
In this video, the pivot point of the dynamic footrests (knee elevation feature) is close to the natural pivot point of the knee.
Dynamic seating – Clinical Applications
Many of the dynamic seating options that are now available were initially designed and used to prevent equipment breakage. Over time, seating and mobility team members also realized that clients were sometimes injuring themselves while moving in their wheelchair due to the intentional or unintentional forces they applied, which could include large and forceful movements.
For many years, wheelchair seating professionals used dynamic seating with a wide variety of clients. This work was instrumental for informing practice. As a result, these professionals observed a wide range of clinical benefits, much of which is supported by research:
- To protect the wheelchair user from injury, including injury from excessive and unrelieved force through joints, contact of the head against the head support pad exceeding concussive forces, and contact of their bodies with broken seating or wheelchair equipment (Lange, 2021).
- To increase sitting tolerance and compliance. Movement can decrease pain and discomfort, prolonging the time a client will tolerate a seated position (Ridilla, et al., 2024; Lyons, et al., 2017; Frank & DeSouza, 2017; Frank et al., 2012; Incoronato, 2007).
- To reduce active extension. By absorbing and diffusing client force, active extension often is reduced in duration and intensity (Cimolin, et al., 2009; Lange, 2021). Imagine sitting behind a client on a mat table as that client begins to extend their hips. If the examiner supports the client’s body and leans back 10 to 20 degrees as the client extends, that force will be diffused, and the client can readily be returned to upright sitting.
- To reduce energy consumption. Some clients with forceful extension and/or large and forceful movements spend a great deal of their day appearing to ‘fight’ their seating system – to the point that they appear to be standing in their wheelchair. This takes a tremendous amount of energy and caloric expenditure (Wang & Raunser, 2023). By diffusing forces through movement, the client can conserve that energy for functional tasks and avoid burning excessive calories.
- To maintain client posture within the seating system (McNamara & Casey, 2007). When a client extends at the hips in a static seating system, this force is not diffused and so results in movement of the client in relation to the support surfaces. For example, as the client extends their hips and pushes their trunk against the back of the seating system, their pelvis migrates forward into a posterior pelvic tilt because there is nowhere else for the pelvis to go. Most likely, the client is unable to correct the position of their pelvis independently and will need repositioning by others.
- To decrease shear forces and pressure. When a client moves in relation to the seating system, shear forces occur as these two surfaces (body and seating) slide across each other (Chen, et al., 2018; Hahn, 2009; Cimolin, et al., 2009). Pressure can be quite high at bony prominences where areas of the client’s body exert the most force against a static seating system, such as the scapulae.
- To increase vestibular and proprioceptive stimulation (Chen, et al., 2018). People need to move, and many clients using wheelchair seating seek sensory input, such as vestibular stimulation, through movement and proprioceptive stimulation from pushing against a resistive surface.
- To increase alertness through movement (Chen, 2018; Phillips, 2017). Most people are more alert when moving and this can be particularly true for some clients using wheelchair seating. For example, people who have a brain injury may be subaroused and movement can increase overall alertness.
- To decrease agitation through movement (Chen, 2018; Phillips, 2017; Pfeiffer, et al., 2008). Agitation can be decreased through body movement. This is common in clients with sensory processing disorders, brain injuries, or dementias.
- To decrease fatigue through movement. (Tanoue, et al., 2016). Just as movement can increase cognitive alertness, fatigue is also improved through movement. Imagine how tiring a long flight is when physical movement is restricted.
- To increase function (Chen, 2018; Phillips, 2017; Adlam, 2015; Dalton, 2014; Cimolin, et al., 2009; Incoronato, 2007). Movement against resistance can improve joint stability (through isometric muscle contraction) and support a body position that increases functional abilities like operating a power wheelchair joystick.
- To increase strength and postural control (Chen, 2018; Phillips, 2017, Adlam, et al., 2014; Hahn, 2009; Cimolin, et al., 2009; Incoronato, 2007). Movement against resistance can increase muscle strength, primarily through isometric muscle contractions (McBurney, et al., 2003; Fowler, et al., 2001). Increased strength, particularly in the trunk, can increase trunk and head control.
- To facilitate active range of motion. Dynamic seating components accommodate movement within a limited range at the hips, knees, ankles, and neck (Adlam, et al., 2014; Cimolin, et al., 2009; Hahn, et al., 2009; Incoronato, 2007).
- To protect wheelchair and seating hardware from breakage or loss of component alignment (Incoronato, 2007; Lange, 2021). Even clients who do not weigh very much are capable of breaking wheelchair components secondary to intermittent or sustained force. Individuals can exert 200% to 600% of their body weight against a static surface because of the high forces they generate from their increased muscle tone (Samaneein et al., 2013).
There are many other benefits that have been observed in clients using dynamic seating, as well. These include improvements in digestion (Incoronato, 2007), vocalization (Adlam, et al., 2014), circulation (Myers, et al., 2021); and social engagement (Adlam, et al., 2015).
Dynamic Seating – Research
The following table summarizes research studies related to clinical phenomena observed in people with cerebral palsy using wheelchair seating and mobility and the impact of dynamic seating on each of these phenomena. Many of these concerns are observed in clients with other diagnoses, as well.
The first column lists common clinical phenomena, the second column summarizes research that supports the presence of each clinical phenomenon, and the third column summarizes research related to dynamic seating and its impact on each clinical phenomenon.
Table 1: Summary of Research Studies
| Clinical Phenomenon | Research that supports this is an issue in CP | Research about DS and this issue |
| Extension / Spasticity | 1. Spasticity increases with resistance, such as client forces exerted against a non-yielding surface (Bar-On, et al., 2018). 2. Clients with increased extension were able to exert up to 200% of their body weight against the back support and up to 600% of their body weight against the foot supports during extension (Samaneein, et al., 2013). | 1. Dynamic Seating decreased extensor thrust (Cimolin, et al., 2009). 2. Dynamic Seating decreased extension patterns (Lange, 2021). |
| Dystonia | 1. Dystonia can lead to pain and discomfort and impact function (Penner, et al., 2013). | 1. Hypothesis proposed that the use of whole-body dynamic seating can improve comfort, activity, participation, and quality of life in young children with dystonic cerebral palsy (Gimeno and Adlam, 2020). This requires more research. 2. Reduced large upper extremity movement and increased smoothness of movement observed in research participants who had the diagnoses of cerebral palsy and dystonia (Cimolin, et al., 2009). |
| Pain | 1. 57 of 133 (43%) of children and adolescents with CP reported having pain in the past 12 months, 17 (30%) reported chronic pain. Participants at GMFC levels IV-V reported more frequent and higher pain intensity. 23% of participants with pain did not receive any treatment. Pain often restricted participation. 2. Four out of six teens with cerebral palsy (GMFCS V) reported pain (Ridilla, et al., 2024). 3. One study of children with cerebral palsy found that nearly 55% of participants reported pain (Penner, et al, 2013) and another study found that 75% of children with cerebral palsy were in pain (Novak, et al., 2012). 4. Comfort is a high priority for families (Gimeno, et al., 2013). 5. Extension forces can lead to pain and, as a result, decrease sitting tolerance (Cimolin, et al., 2009; Incoronato, 2007). 6. Of people with CP, 75% experience chronic pain (CPARF.org). 7. Adults with CP are more likely to experience joint pain compared to non-disabled adults (43.6% vs. 28.0%) (Peterson, et al., 2015). 8. Children with dystonia report pain as a common concern (De Knegt, et al., 2013; Gimeno, et al., 2013; Penner, et al., 2013). 9. Pain may lead to decreased function and mobility (Haak, et al., 2009). 10. One study concluded that over half of the participants who had spastic CP reported problematic pain. The participants were individuals with CP GMFCS levels IV and V who used power wheelchairs (Frank, et al., 2017). | 1. The Ridilla, et al. study (2024) indicated an increase in self-relief of pressure after prolonged seating in a response to increased pain. 2. Frank, et al. (2012) found that most power wheelchair users in their study experienced pain and that one strategy that reduced pain was changing position. 3. Movement has been shown to decrease pain in wheelchair users (Lyons, et al., 2017; Frank & DeSouza, 2017). 4. Incoronato (2007) found a reduction in pain with use of a specific dynamic seating system in a retrospective study. |
| Arthritis | 1. Adults with CP are more likely to experience arthritis compared to non-disabled adults (31.4% vs. 17.4%, Peterson, et al., 2015) (Whitney, et al., 2018). 2. Arthritis may lead to decreased function and mobility (Haak, et al., 2009). | These studies could form the basis for future research to determine if dynamic seating could diffuse extensor forces to specifically lessen forces occurring in the joints. |
| Injury (from extensor forces, often from forceful contact with equipment or with damaged equipment) | 1. The forces from extension on the client’s body can lead to injury (Hong, 2006, Lange, 2021). | 1. Further injuries were prevented in a client using dynamic seating who had a history of injuries secondary to extreme extension forces (Lange, 2021). |
| Shear forces (from client moving in relation to seating support surfaces) | 1. Cimolin et al. (2009) used quantitative movement analysis to compare movement during extensor thrust using a dynamic back support and using a rigid back support and found increased vertical trunk movement (shear) during extension with the rigid back support. | 1. Cimolin et al. (2009) used quantitative movement analysis to compare movement during extensor thrust using a dynamic back support and using a rigid back support and found decreased vertical trunk movement (shear) during extension with the dynamic back support. 2. Dynamic Seating allows movement while maintaining contact with the support surfaces, providing stability, and reducing shear forces (Hahn, 2009; Cimolin, et al, 2009; Chen, et al., 2018). |
| Equipment Breakage (secondary to strong sustained and/or intermittent client forces) | 1. The forces from extension on a static wheelchair seat and frame can be so strong as to cause damage to equipment (Hong, 2006). 2. Breakage frequently occurs at the foot supports, leg support hangers, back support mounting hardware, and head support hardware (Hahn, 2009). 3. Continuous rocking, as well as forceful rocking, can lead to damage of the wheelchair seating system and frame (Incoronato, 2007). | 1. Dynamic seating is designed to absorb extreme forces, which in turn, protects the wheelchair seating and frame from wear and tear and even breakage (Incoronato, 2007). 2. A single subject using dynamic seating experienced no further equipment breakage once receiving this intervention, despite a long history of equipment breakage (Lange, 2021). |
| Lack of movement (secondary to degree of postural support required within a seating system) | 1. Many people using wheelchair seating and mobility cannot move their bodies significantly in relation to the seating system. This may be due to motor limitations or the postural supports themselves (Strobl, et al., 2013). | 1. Movement can calm (reduce agitation), arouse (increase alertness), strengthen muscles, enhance visual control, and provide comfort, as well as improve voluntary functional movements (Chen, 2018; Phillips, 2017) by varying our position. 2. Maladaptive behaviors may be reduced in response to movement (Pfeiffer, et al., 2008). 3. Rollo, et al. (2017) reviewed 5 studies and found that classroom based dynamic seating improved attention. 4. Self-directed movement increases brain derived neurotrophic factor (BDNF) which enhances brain recovery at the structural and chemical level and encourages dendrite and axon development (Phillips, et al., 2017). Dynamic Seating may, through self-directed movement of the dynamic components, impact brain recovery, development, and function. |
| Decreased postural control, stability, and function | 1. Motor development plateaus for children with CP as early as 3 years of age with one out of three children unable to gain adequate trunk control for stable, independent sitting (Beckung, et al., 2007; Rosenbaum, et al., 2002). The estimated limit of development decreased as severity of impairment increased (Rosenbaum, et al., 2002). | 1. Dynamic Seating allows movement while maintaining contact with the support surfaces, providing stability, and reducing shear forces (Chen, et al., 2018; Hahn, 2009; Cimolin, et al, 2009). 2. Adlam, et al. (2014) found increased head control and increased symmetry in posture using a dynamic seating system. 3.Incoronato (2007) noted improved posture in their study. 4. McNamara & Casey (2007) found improved overall positioning, including reduced sacral sitting (related to seat inclination). 5. Adlam (2015) found increased function with use of a dynamic seat in one study and in another (2014) one subject was able to access a switch when using dynamic seating. 6. Incoronato (2007) found improvement of motor control of the upper extremities, trunk, and head. 7. Dalton, (2014) found increased head and arm control with a simulated dynamic foot support. 8. Cimolin, et al. (2009) noted increased smoothness of movement. 9. Movement can increase vestibular and proprioceptive stimulation which can improve stability (Chen, et al., 2018). 10. Movement against resistance has been demonstrated to increase strength in people with increased muscle tone (McBurney, et al., 2003) without an increase in spasticity (Fowler, et al., 2001). |
| Range of motion losses (often secondary to prolonged time in a position, such as sitting in a wheelchair) | 1. Range of motion may decrease secondary to a prolonged seated position (Strobl, et al., 2013). | 1. Increased range of motion and movement was found when using dynamic seating (Adlam, et al., 2014; Cimolin, et al., 2009; Hahn, et al., 2009; Incoronato, 2007). |
| GI issues (including reflux, digestion, and constipation) | 1. Children with CP are prone to digestive issues such as upset stomach, vomiting, bloating, and constipation (Sullivan & Andrew, 2017). | 1. Dynamic seating improves digestion (Incoronato, 2007). |
| Decreased vocalization | 1. Speech Problems affect more than half of children with CP (based in Sweden, Nordberg, et al., 2013). | 1. Dynamic seating improves vocalization (Adlam, et al., 2014). |
| Decreased circulation, often secondary to prolonged sitting | 1. Patrangenaru (2006) noted that static seating can lead to circulation-related issues. | 1. Increasing movement improves circulation and has health benefits (Myers, et al., 2021). |
| Decreased social engagement and participation | 1. Children with CP have less participation and enjoyment of social and recreational activities compared to typically developing children (Chiarello, et al, 2014). | 1. Adlam, et al. (2015) found increased social engagement with dynamic seating intervention. |
Funding Challenges
The Centers for Medicare and Medicaid Services (CMS) approved Healthcare Common Procedure Coding System (HCPCS) Level II code E2398 “Wheelchair accessory, dynamic positioning hardware for back,” effective January 1, 2020. A Preliminary Medicare Payment Determination was made in May of 2022, comparing the E2398 code for a dynamic back to the E1015 code for a “Shock Absorber for Manual Wheelchair.” One way CMS determines a fee schedule is by conducting a ‘cross walk’ that compares an item like the dynamic back to another coded item that already has a fee schedule. The payment determination for the code is then based upon the cost of the item that already has a fee schedule. As a result, the proposed reimbursement rate for the dynamic back was between $152.55 to $183.02, far below the cost to manufacture it. Despite significant advocacy efforts to change the fee schedule to a more reasonable reimbursement rate, the new payment schedule went into effect April 1, 2024. Industry leaders must continue to advocate for change, to ensure that those who require this intervention can still receive it.
A paradigm shift: Movement for all
Many people using wheelchair seating can independently move within their seating system and then return to an optimal position. This provides variety in their body position, which is important for functional tasks as well as for moving joints and muscles. Our brains are wired to move. Movement within an office chair or a wheelchair seating system provides many benefits like increasing alertness (Chen, 2018; Phillips, 2017), reducing discomfort (Ridilla, et al., 2024), and accommodating different body positions for specific tasks (Adlam, 2015; Adlam, 2014). For someone in a wheelchair seating system, pressure may also be relieved and/or redistributed (Ridilla, 2024).
Some people using wheelchair seating can move within their seating system, yet they are not able to independently return to an optimal position. This is typically because their movement causes them to push off a non-yielding surface, such as the back support during hip extension. This movement can cause their pelvis to move forward and into posterior pelvic tilt. As another example, individuals may push against their footplates with active knee extension, causing their pelvis to elevate off the cushion and then return to the seating surface in a poor posture. This person may lack the ability to reposition their bodies into optimal alignment after movement without assistance from a caregiver.
In these situations, movement can be provided through dynamic seating without the resultant loss of position. For example, when a client pushes against the back support during hip extension, a dynamic back moves in response, diffusing force and reducing leverage so that the client’s body stays in alignment with their seating supports until they return to their starting position. If the client is pushing against the footplates, dynamic footrests move in response to this force. As the dynamic footrests move, they diffuse the client’s forces and reduce leverage so they can extend their legs without loss of pelvic position.
Importantly, dynamic seating can provide movement, even within a very aggressive and restrictive seating system. Some clients may not be able to move their hips in relation to their seating system secondary to restrictive seating; however, a dynamic back allows hip extension without loss of position. A client may not be able to move their feet off the footplates secondary to seating interventions such as shoe holders with strapping, however the client can extend their knees and ankles using dynamic footrests (see Figure 4 below).

Movement as a Human Right
Is a person’s right to move being neglected when we provide aggressive seating interventions to maintain posture, yet those supports prevent the individual from moving?
Instead of providing postural support OR providing movement, can postural support AND movement be provided? Just as mobility is considered a human right (Sabet et al., 2022), we argue that movement is as well. Service members can, and should, provide movement for individuals within a wheelchair seating system so they can experience the health and functional benefits that movement offers. While many people using wheelchair seating can move within their seating system and reposition their bodies independently, others cannot. They may be restricted from moving by their seating supports, and/or unable to reposition their bodies after they move. Dynamic seating is an important solution to this ‘either-or’ dilemma because it helps clients maintain their position while also accommodating their movements.
Summary
Although dynamic seating first became commercially available in 1989, a variety of options did not emerge until the early 2000s. Initially designed to prevent equipment breakage, dynamic seating has a wide variety of clinical applications. Client and caregiver experiences, expert clinical consensus, and research support these benefits and innovative clinical applications. Product design has changed over the years to provide more efficient responses to client forces and minimize loss of client position in relation to the support surfaces during movement. In a continued innovation of thought, seating and wheeled mobility team members must consider provision of movement within a seating system as a human right. This is particularly true for clients with the inability to change their position without a loss of alignment with their seating support surfaces.
Please refer to a prior Rehab Case Study on the application of dynamic seating with a young child here.
Click here to open a list of references in a new tab.

Michelle may be reached at MichelleLange1@outlook.com or 720-333-2661. Michelle Lange is an occupational therapist with over 38 years of experience and has been in private practice, Access to Independence, for over 19 years where she currently focuses on education and consultation. She is a well-respected lecturer, both nationally and internationally, and has authored numerous texts, chapters, and articles. She is the co-editor of “Seating and Wheeled Mobility: A Clinical Resource Guide (1st & 2nd eds).” Michelle is a RESNA Fellow and member of the Clinician Task Force. She is a RESNA certified ATP and SMS.

Becky Breaux may be reached at Becky.Breaux@ucdenver.edu or 303-315-0601. Rebecca (Becky) Breaux, PhD, OTR/L, ATP is an Assistant Research Professor and occupational therapist at the Center for Innovative Design and Engineering, CU Denver. As a clinician, she has 30 years of clinical experience, providing assistive technology assessments and training to children and adults with disabilities in the areas of seating and wheeled mobility and access to technologies. Her research explores factors that influence the best practices in the provision of Complex Rehabilitation Technologies, and the impact of under-utilized technologies on user experiences and outcomes.